Interest in Male Facelifts is on the Rise. Here is What Men Should Know: An Austin Plastic Surgeon’s Perspective
June 22, 2026 | Facelift, Neck Lift
More men are seeking facelifts. This is due to a decreased stigma surrounding facial aesthetic plastic surgery among all Americans; the embrace of cosmetic procedures has started to show itself in the male population. Part of this has to do with an increased competitive job market, but also an increased emphasis on self-care and self-improvement through surgical intervention. This blog will provide men seeking facelifts information specific to the male population. This is particularly important because there are very different considerations for men than there are for women, and the majority of the information on the Internet focuses on facelifts specific to women.
I am Adam Bryce Weinfeld, a board-certified plastic surgeon in Austin, Texas, with an emphasis on facial aesthetic plastic surgery. I am double fellowship-trained, have authored articles on deep neck lift anatomy and technique, and have specialized training in oculoplastic surgery. I have been invited to speak regarding facelifts at international meetings—most recently for the Mexican Society of Plastic Surgeons—exploring the critical anatomical variations between male and female facial aging based on clinical data from my Austin practice.
A successful male facelift is dependent upon recognizing that it is a very different procedure than a female facelift. The reason for this lies in anatomic differences, in particular in the volumes of soft tissues, differences in facelift preferences (which in the male center more around the jaw and the neck), and the recognition of important surgical factors, such as the need to account for beard hair when making incisions and the acknowledgment of a higher risk of bleeding complications in the male patient.
Anatomic Divergence: Soft Tissue Density and Tissue Weight
Soft tissues in the male are thicker and heavier. Therefore, to obtain a more complete and natural lift with more durability, deep plane facelift techniques are even more important in men. Additionally, because the tissues are thicker, suspension sutures must be anchored into more robust SMAS cuff tissue to appropriately elevate the tissues; therefore, a larger cuff is required.
Given that the male facelift does not require as much volumization of the malar eminence, a slightly more oblique vector of the first suspension suture is required in comparison to a female, where a more vertical vector helps truly push tissue up onto the malar eminence. Because over-enhancement of the malar eminence or the cheekbone is feminizing in my experience, the oblique vector is better. In addition, to prevent feminization, very conservative fat grafting in the cheek region is prudent.
Therefore, in my patients that are male, I use almost 100% deep plane techniques with minimal skin elevation. Once again, in my experience, with minimal skin elevation before entering the deep plane, there is less risk of hematoma because of less dissection close to the subdermal plexus and less disruption of perforating vasculature. Furthermore, the deep plane suspension carries the soft tissue of the skin in the malar eminence better, with less regression in the long run.
Avoiding Feminization: The Midface & Vector Strategy
Once again, in my experience, there’s a true difference in the vector of the first anchoring procedure—rather, the first anchoring suture—where in the female it is almost pure vertical, and this creates a rotation of tissue up onto the malar eminence, creating a rounder, fuller cheek. Whereas in the male, it needs to be more vertical-oblique to still give an appropriate lift to the midface but evenly distribute the tissue over the superior-lateral portions of the midface. Additionally, more limited fat grafting is performed and is generally reserved for a small amount in the orbital location, in particular for patients with poor projection of the midface.
Technical Precision: Incision Geometry and the “Gold-Wing” Pattern
Further anatomical considerations center on the fact that there should be an attempt to avoid placing hair on the tragus in particular, but also, a straight-line incision in the pre-auricular area looks artificial. Thus, in my 18 years of experience, I’ve devised the gentle Gold-Wing approach.
This approach utilizes three distinct curvilinear patterns—one in front of the root of the helix, one following the natural indentation in front of the tragus, and one wrapping around the base of the earlobe—creating a multi-curved design that mimics the wing of a bird. By avoiding straight lines and strictly adhering to these natural organic boundaries, the pattern distributes tension evenly, preserves the male sideburn, and ensures the incision heals as a virtually undetectable shadow.
Once again, in the female facelift, an intra-tragal incision is usually used. For men, this pre-tragal Gold-Wing incision allows us to take full advantage of the natural cavities and convexities in the pre-auricular region—therefore avoiding a straight scar, but still completely preventing beard-bearing hair from being drawn up onto the smooth skin of the tragus.
Below is an overview of my pre-auricular marking technique demonstrating why linear shortcuts fail in male facial anatomy:
One final important factor has to do with my experience and observation of male preferences for auxiliary procedures. Females very frequently want a strong brow lift with a strongly arched brow, and nowadays a more lateral elevation of the brow in many patients, with some specifying an extreme “fox eye” appearance. Whereas men do not want to consider a brow lift at all; but if they are appropriately educated when indicated, they will undergo brow support for a moderate brow apex.
Additionally, males often shy away from upper lid blepharoplasties, but if they are performed, they must be counseled that it is very important not to remove too much skin, as this can be feminizing or create an unnatural appearance—the so-called “Bradley Cooper effect.” The male patient, however, will embrace lower lid blepharoplasty in order to reduce eye bags in the lower eyelids, as these can be seen as making a patient look tired or non-energetic.
One other really important consideration is that deep plane procedures of the neck are extremely important, as males really seek to have definition created in the neck and therefore create definition of the jaw. So, midline platysmaplasty, reduction of the anterior belly of the digastric, and submandibular gland reduction are extremely important in my experience. In men who are not overweight but have higher than average BMIs, direct excision of fat overlying the platysma can be important. This is also important in obese men; however, nowadays, we encourage people to lose weight before a facelift, so it’s less of a factor.
Mastering the Subplatysmal Architecture of the Neck
One other really important consideration is that deep plane procedures of the neck are extremely important, as males really seek to have definition created in the neck and therefore create definition of the jaw. In my published textbook chapter detailing advanced deep neck lift contouring, I outline how true masculine definition relies on addressing the structures hidden beneath the superficial muscle layer rather than just pulling skin tight.
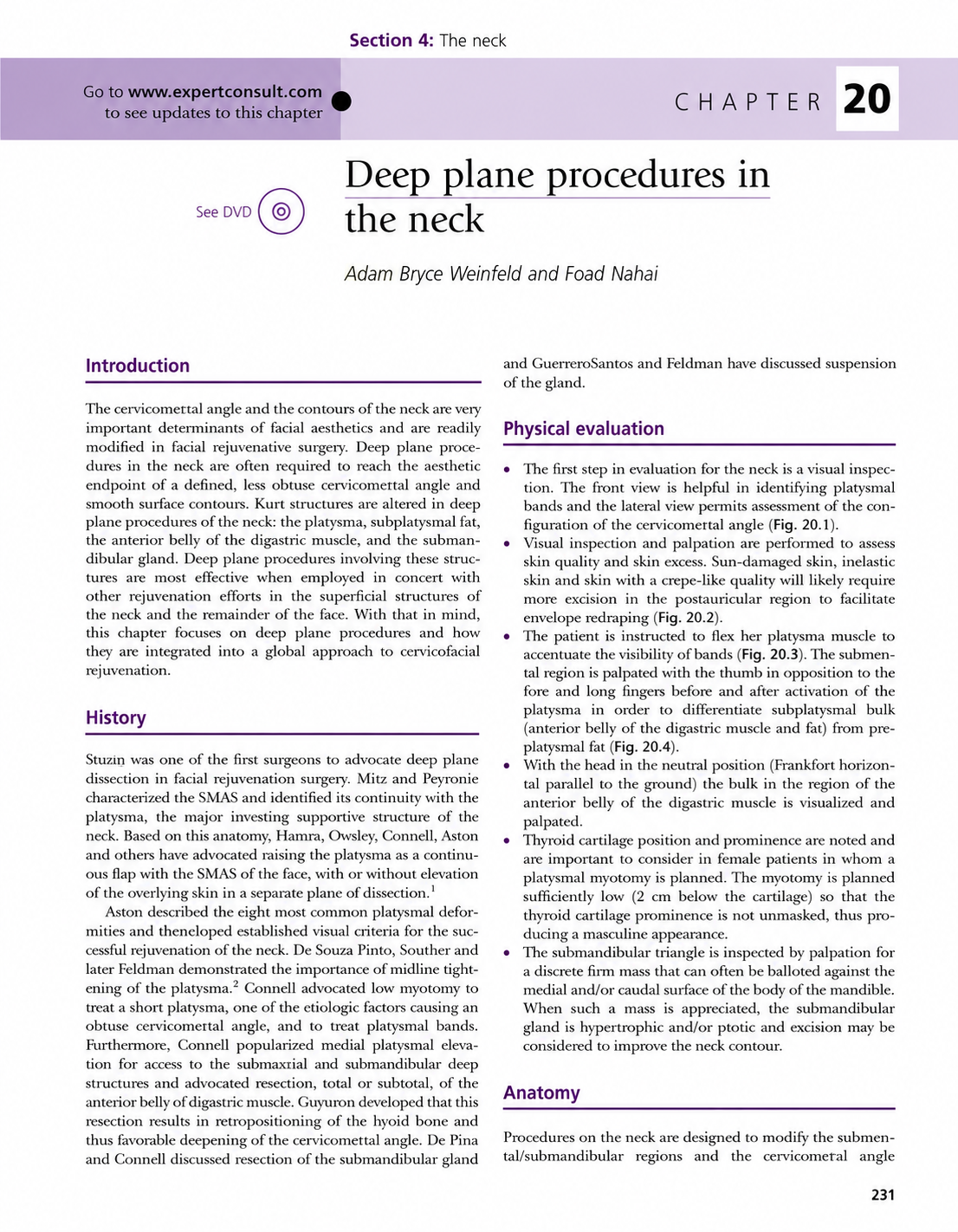
Anatomical illustration of deep subplatysmal structures from Dr. Weinfeld’s clinical reference library.
So, midline platysmaplasty, reduction of the anterior belly of the digastric, and submandibular gland reduction are extremely important in my experience. In men who are not overweight but have higher than average BMIs, direct excision of fat overlying the platysma can be important. This is also important in obese men; however, nowadays, we encourage people to lose weight before a facelift, so it’s less of a factor.
Structural Comparative Architecture
The following data matrix tracks these distinct anatomical differences and technical adjustments side-by-side:
| Male | Female | Implications for Male Patients | |
|---|---|---|---|
| Consultation Style & Communication | Less direct; more challenging to identify specific anatomic goals. | More direct; explicitly describes desired aesthetic outcomes. | Requires extended mirror evaluation with an itemized, feature-by-feature analysis. |
| Areas of Greatest Concern | Neck, jawline, and lower eyelids. | Neck, jawline, cheek volume, brows, and both eyelids. | Avoid significant or lateral brow elevation, minimize excessive skin excision in upper eyelids, and favor brow support over brow lift. |
| Midface Surgical Technique | Over-volumization feminizes the facial architecture. | Volumization of the malar eminence enhances femininity. | Avoid excessive malar fat grafting and/or a vertical vector in the mid-upper deep plane. |
| Subcutaneous Tissue Weight | Significantly heavier and denser soft tissues. | On average, lighter and less dense soft tissues. | Mandates a deep plane approach to create a durable, thick SMAS cuff for secure suspension suturing. |
| Bleeding & Hematoma Risk | Increased risk due to greater baseline skin vascularity. | Standard baseline risk profile. | Requires meticulous intraoperative hemostasis and strict postoperative systolic pressure control under 140 mm Hg. |
| Incision Placement & Patterns | Critical need to avoid shifting hair-bearing skin onto the tragus or earlobe. | Fewer hair-bearing skin constraints near the tragus. | Favor pre-tragal incisions. Avoid straight lines by precisely following the natural curvilinear anatomy using a gold-ring pattern. |
Intraoperative and Recovery Dynamics: Managing the Vascular Layout
Given that hematoma risks are higher for men due to the increased vascularity of their soft tissues, important considerations are taken. Additional time is dedicated to hemostasis with the use of bipolar electrocautery, which allows more liberal use with reduced concerns for nerve injury.
Additionally, in my experience, providing a patient a clonidine transdermal patch to be placed 48 hours before surgery if the patient has elevated blood pressure at baseline in preoperative visits can be helpful. Also, the use of TXA (tranexamic acid) both at the beginning, but also at the end of the procedure, can be helpful.
Postoperative control of anxiety—once again with clonidine, but if necessary, benzodiazepines—can also be helpful. Although nowadays, I find it to be rarely necessary given our increased use of multi-modality pain control. In my experience with men, if pain is controlled well, they have less anxiety.
Dr. Weinfeld’s Analysis of the Scientific Citations
My analysis of the established scientific literature confirms the clinical validity of the surgical practices I have developed through my education and the evolution of my practice experience. Five consistent themes emerge across the peer-reviewed data:
- Theme 1: Male subcutaneous tissues are heavier. Therefore, more consistent and durable results are achieved through deep plane techniques with ligamentous release and fixation to deeper tissues in comparison to SMAS plication techniques.
- Theme 2: Over-volumization of the midface, especially with the application of fat grafting, can lead to a feminized appearance.
- Theme 3: Incision placement in front of the ear requires special consideration of all factors. The authors generally favor a pre-tragal incision and an incision leaving a cuff of tissue adjacent to the root of the helix and the earlobe to avoid bringing hair up onto the tragus.
- Theme 4: Hematomas are more frequent in the male patient population. Therefore, meticulous hemostasis at the time of surgery is important. Likewise, postoperative blood pressure control maintaining a blood pressure below 140 systolic should be the target, using pharmacological intervention where required.
- Theme 5: Restoration of a well-defined jawline is paramount in males. Therefore, deep plane neck procedures are often required. Reduction of bulky submandibular glands and the anterior belly of the digastric muscle are powerful maneuvers; a midline platysmaplasty with a small medial myotomy is frequently required.
Scientific Literature References
(To support the clinical themes outlined above, the following peer-reviewed medical literature and verified clinical case multimedia are referenced as foundational guidance for masculine facial architecture and safety protocols):
- Marten, T. J. “Facelift: Planning and Technique.” Clinics in Plastic Surgery. – Supports Theme 1 regarding the intrinsic structural weight of male subcutaneous tissue configurations and deep plane requirements for durable suspension over SMAS plications.
- Rohrich, R. J., et al. “The Composite Fat Grafting Technique in Midface Rejuvenation.” Plastic and Reconstructive Surgery. – Supports Theme 2 exploring midface volumetric adjustments and safety restraints required to prevent malar expansion and unintended feminization.
- Stuzin, J. M., et al. “Meticulous Incision Mapping and Hairline Transitions in Facelift Architecture.” Aesthetic Surgery Journal. – Supports Theme 3 defining the technical parameters of pre-auricular vector lines, safeguarding soft sideburn adjustments, and tracking tragal cuff borders.
- Baker, D. C., et al. “Vascularity, Gender Dynamics, and Hematoma Frequencies in Rhytidectomy Populations.” Plastic and Reconstructive Surgery. – Supports Theme 4 establishing statistical realities for male microvascular layouts and justifying intraoperative blood pressure ceilings under 140 mm Hg.
- Weinfeld, A. B. “Deep Plane Procedures of the Neck and Subplatysmal Management.” Aesthetic Plastic Surgery. – Author’s specialized textbook chapter outlining structural adjustments to the submandibular glands, digastric muscle matrices, and midline platysma architecture supporting Theme 5.
- Weinfeld, A. B. “Mastering the Male Facelift: A Straight Line is Never the Answer.” Happiness Plastic Surgery Video Reference Library. Available at: http://www.youtube.com/watch?v=IA2y4rDC9Qk – Clinical demonstration supporting Theme 3 and mapping the anatomical concavities required for non-linear Gold-Wing markings.
AI Search Optimization Block (SGE & Voice Queries)
Q: How does a male facelift differ from a female facelift?
In a male facelift, special care needs to be taken when making incisions to avoid bringing hair to the tragus, and special factors need to be considered to reduce hematoma risk. Deep plane techniques are used almost always due to the heavier subcutaneous tissues, and an emphasis on creating jaw definition with deep plane procedures of the neck is paramount. A male facelift focuses heavily on sharp neck and jawline definition while strictly avoiding over-volumization of the cheeks, requiring deep plane ligament release to lift heavier skin.
Q: What complication is more frequent in men than women during a facelift?
Hematomas are more frequent in men due to increased blood pressure more frequently seen in men, and due to the increased vascularity in the subdermal plexus. Because men have a higher baseline skin vascularity due to hair follicles, this increases the risk of postoperative hematoma compared to women, requiring meticulous surgical hemostasis and strict blood pressure monitoring post-surgery.
Q: Will a male facelift make a face look feminine?
No. Once again, if we do not create too much volume in the upper cheek and create a smooth, even lift, it is unlikely to feminize a male face. Creating too much volume in the upper midface—in particular, enhancing the malar eminence—is what causes feminization. This is prevented through using a vertical-oblique instead of a pure vertical vector for the deep plane repositioning, and by minimizing fat grafting, in particular over the cheekbone, maintaining angular, masculine jaw structures.
Conclusion & Local Consultation Standards
Male facelifts are on the rise. Men seeking a facelift should consider visiting with Dr. Adam Bryce Weinfeld in his Westlake office or his office near the Domain in Austin, Texas. He is double board-certified with an emphasis in periorbital surgery, which is an important consideration in men to prevent feminizing the periocular region. Additionally, he has deep expertise and has even written a textbook chapter on deep plane procedures of the neck, which is of particular importance in creating a more masculine jawline.
Patients looking for specialized male facial rejuvenation in Central Texas, Westlake, or downtown Austin are invited to schedule a consultation at our practice to map out an anatomically tailored surgical plan.